OrthoNeuroSpine & Pain Institute
OrthoNeuroSpine & Pain Institute
Cervical, Thoracic, Lumbar, Sacral, Sacroiliac Spine
Comprehensive, Compassionate & Holistic Care
Nonoperative & Operative Management
Multidisciplinary Biopsychosocial Approach

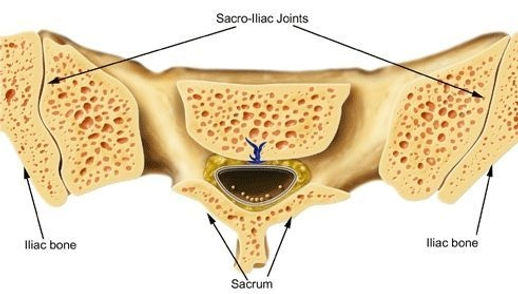
Sacroiliac Joint Anatomy and Function
The sacroiliac joint is located in the pelvis, linking the iliac bone (pelvis) to the sacrum (lowest part of the spine above the tailbone). This joint transfers weight and forces between your upper body and legs. It is an essential component for shock absorption to prevent impact forces during walking from reaching the spine.
The sacroiliac joint is stabilized by a network of ligaments and muscles, which also limit motion. The normal sacroiliac joint has a small amount of normal motion of approximately 2-4 mm of movement in any direction. The sacroiliac ligaments in women are less stiff than in men, allowing the mobility necessary for childbirth.
The sacroiliac (SI) joint is the largest axial joint in the body, with an average surface area of 17.5 cm2 There is wide variability in the adult SI joint, encompassing size, shape, and surface contour. Large disparities
may even exist within the same individual
The SI joint is most often characterized as a large, auricular-shaped, diarthrodial synovial joint. In reality, only the anterior third of the interface between the
sacrum and ilium is a true synovial joint; the rest of the junction is comprised of an intricate set of ligamentous connections. Because of an absent or rudimentary posterior capsule, the SI ligamentous structure is more extensive dorsally, functioning as a connecting band between the sacrum and ilia. The main function of this ligamentous system is to limit motion in all planes of movement. In women the ligaments are weaker, allowing the mobility necessary for parturition.
The SI joint is also supported by a network of muscles that help to deliver regional muscular forces to the pelvic bones. Some of these muscles, such as the gluteus maximus, piriformis and biceps femoris, are functionally connected
to SI joint ligaments, so their actions can affect joint mobility. The potential for vertical shearing is present in approximately 30% of SI joints, owing to the
more acute angulation of the short, horizontal articular component
Age-related changes in the SI joint begin in puberty and continue throughout life. During adolescence, the iliac surface becomes rougher, duller, and coated in
some areas with fibrous plaques. These senescent changes accelerate during the third and fourth decades of life and are manifested by surface irregularities, crevice formation, fibrillation and the clumping of chondrocytes.
Degenerative changes on the sacral side generally lag 10–20 yr behind those affecting the iliac surface. In the sixth decade, motion at the joint may become markedly restricted as the capsule becomes increasingly collagenous
and fibrous ankylosis occurs. By the eighth decade of life, erosions and plaque formation are inevitable and ubiquitous
The innervation of the SI joint remains a subject of much debate. The lateral branches of the L4-S3 dorsal rami are cited by some experts as composing the major innervations to the posterior SI joint